
![]()
![]()
1 Yusuf Karaşin
2 Tuğba Öz
3 Yalçın Karagöz
1 Istanbul Gedik University, Gedik Vocational School, Department of Medical Services and Techniques, İstanbul, Türkiye
2 Istanbul Beykent University, Faculty of Health Sciences, Department of Nursing, İstanbul, Türkiye
3 Düzce University, Faculty of Business Administration, Department of Health Management, Düzce, Türkiye
Article received: 29.08.2024.
Article accepted: 25.11.2024.
https://doi.org/10.24141/2/8/2/9
Author for correspondence:
Yusuf Karaşin
Istanbul Gedik University, Gedik Vocational School, Department of Medical Services and Techniques İstanbul/Türkiye
E-mail: yusuf.karasin@gedik.edu.tr
![]()
Keywords: Caesarean section, attitude scale, scale development, Turkey
![]()
![]()
Introduction. Caesarean section is an alternative to normal birth and is performed through an incision. Caesarean section can be a method applied in cases of necessity, but it can also be applied in cases where it is not mandatory.
Aim. The aim of this study is to determine the at- titudes of women towards caesarean section. Methods. In this regard, 437 women of reproductive age between 18-49 residing in Esenyurt district of Istanbul province were included in the study. In the study, a 42-question survey was first drafted. After receiving expert opinion and conducting a pilot study, a draft survey consisting of 32 questions was applied to the participants in person. Firstly, explanatory fac- tor analysis was applied to the data. Following the analysis, 12 questions that were not collected under any dimension were removed from the scale and 5 factors including 20 questions were found. After this stage, Confirmatory Factor Analysis was applied to the identified factors.
Results. It was determined that the model obtained was a perfect fit for the data. Therefore, the scale developed by exploratory factor analysis was con- firmed by confirmatory factor analysis. The Cron- bach’s coefficient of the developed scale was cal- culated as 0.820 and it was concluded that it was highly reliable.
Conclusion. It was decided that the developed scale could be used to measure women’s attitudes towards caesarean section.
![]()
![]()
In general, the process of removing the child from the mother’s womb by performing a surgical intervention other than natural birth is called cesarean section. This surgical intervention may be due to obligatory reasons or non-obligatory reasons. The non-obliga- tory reasons include, inter alia, the mother’s choice of cesarean section upon her own request, physician guidance, history of miscarriage, and fear of birth (1-6). While the World Health Organization considers the rate of cesarean section in the range of 10-15% to be acceptable according to the standards set by it, it is seen that the cesarean section rate is much high- er than the desired level in many countries, including Turkey. This brings a serious financial burden to the country’s health system (7). When the literature is examined in the Turkish sample, it is possible to see that there are various studies on cesarean section (2, 8-10). This study differs from the studies in the literature. The fact that the attitude scale towards caesarean section has not been directly included in the literature by sampling women between the ages of 18-49 in the fertility category in studies involv- ing the Turkish sample reveals the unique aspect of this study. The aim of this study is to introduce the factors affecting attitudes towards cesarean section into the literature in the Turkish sample.
Pregnancy and subsequent birth cause several phys- ical and psychological changes in women’s lives. Al- though labour is a natural process, the interventions applied negatively affect the course of labour and may cause problems in some cases. To prevent all the negative effects that may occur in labour, it is important to choose the method of delivery carefully in terms of both mother and baby health (11). One of the existing delivery methods other than normal delivery method is caesarean section.
It is seen that there are many definitions of caesarean section. According to one definition, caesarean sec- tion is a major abdominal surgery performed on wom- en in both developed and underdeveloped countries
(12). Veef and Van de Velde (2022) define caesarean section as a surgical operation performed worldwide
(13). Caesarean section is an important maternal
health service (14). Caesarean section is defined as a preferred mode of delivery in cases where vaginal delivery is not possible or is risky for the mother or fetus (10-11). When the history of caesarean section is examined, it is seen that it has been used since ancient times and is a part of human culture (15). The term caesarean section is derived from the Latin word ‘caederal’ meaning ‘to cut’. It is narrated that it was first applied during the Roman period to extract the baby in the last trimester of pregnancy from the mother’s womb (16).
The indications for caesarean section are listed as multiple pregnancies, presentation disorders, mater- nal medical problems, presence of infection that can be transmitted from mother to baby, placental disor- ders such as placenta previa or ablatio placentae, fe- tus weighing 4.5 kg due to maternal diabetes, history of shoulder dystocia, Cephalopelvic disproportion, pre- vious uterine surgery and maternal request (17-18).
Caesarean section rates have increased significantly over time. The optimisation of caesarean section rates is a global priority. Excessive caesarean sec- tions can lead to poor outcomes for both mother and child (7,19-20). In addition, high rates of caesarean section are considered a public health problem world- wide (21). Although caesarean section is seen as a life-saving surgery for mother and fetus, when nec- essary, it also carries various risks as in all surgical in- terventions (22-23). Complications such as bleeding, need for blood transfusion, increased risk of uterine rupture and pelvic infections may develop during or after caesarean section. Caesarean section increases the length of hospital stay and causes urinary tract injuries, anaesthesia complications and thromboem- bolic events. Caesarean section may also adversely affect breastfeeding, as there may be a delay in the bringing together of mother and baby. In addition, challenges in adapting to the role of motherhood af- ter caesarean section, prolongation of the mother’s recovery period, and difficulties associated with the care of the mother and the baby are also complica- tions of caesarean section (24).
The rates of caesarean sections in developed and emerging countries are not encouraging at all. The World Health Organisation (WHO)’s recommendation for caesarean section rates is 10-15%. In the last 25 years, it has been reported that there has been an in- crease of over 30% in caesarean section rates in Egypt, Dominican Republic, China, Georgia and Turkey (25). According to 2015 WHO’s data, Brazil with 55.6%, Do-
minican Republic with 56.4%, Turkey with 50.4%, Iran with 48%, China with 47% and Egypt with 51.8% are the five countries with the highest caesarean section rates. In the same year, Turkey ranked first in caesar- ean section rates among OECD countries (26). When the caesarean section in Turkey Health Statistics is analysed, the following rates are obtained: 51.1% in 2014; 53.1% in 2015-2016-2017; 54.9% in 2018;
54.4% in 2019. It is seen that the caesarean section rates in Turkey are considerably higher than the rec- ommendation of the WHO’s caesarean section rate. The reasons for this dramatic increase today are list- ed as increased age at first pregnancy, continuous ap- plication of fetal monitoring, the misconception that cesarean delivery is safer for the baby, the increase in the socio-economic level of families, mothers’ desire for a painless, effortless birth, and physicians’ guid- ance for caesarean delivery. The reasons why women prefer caesarean section are factors such as fear of normal delivery, lack of adequate information about normal vaginal delivery, women’s fear and avoidance of birth pain, inadequate conditions in the delivery room, lack of adequate psychological support during labour and offering the option of epidural anaesthe- sia. Unfortunately, caesarean section is perceived as a comfortable delivery method by families, society and physicians (27). Perner et al. (2022) examined the caesarean section rates and social inequality in 305 cities in the Latin American region including Bra- zil, Colombia, Guatemala, Mexico and Peru, and found that there is a relationship between the mother’s education level, age and gross domestic product and caesarean section rates (28). In another study con- ducted by Okyere et al. (2022), the caesarean section rates of women were analysed based on official data in Gana between 1998-2014. After the examination, it was concluded that factors such as the city of resi- dence, gross domestic product and education affect caesarean section (29). In the study performed by Özkan et al. (2013), 1159 women between the ages of 18-49 with a history of pregnancy were included in the sample. It was determined that 43.2% of wom- en gave birth by cesarean section. Factors affecting the situation of having a cesarean section were de- termined as the mother’s living in the city, her last birth in the private sector, physician referral, and com- pulsory cesarean section. In addition, the fact that women are not fully informed about cesarean section is another factor that increases the risk of cesarean section (1). One of the factors affecting the choice of cesarean section is that the day when the baby will
be born is determined in advance by cesarean sec- tion. Couples can choose a cesarean section to have the child on the day they plan. In the study performed by Liang et al. (2018) which included 1169 pregnant women, it was found that only 8% of pregnant wom- en had a preference for cesarean section, and when the factors affecting this situation of pregnant wom- en who preferred cesarean section were examined, it was found that the most important factor was the desire for the baby to be born on a special day. Other factors are the couples’ desire for this option and the fact that cesarean section is less painful than vagi- nal birth (30). Fuglenes et al. (2011) used the data of the mother-child study, which included a sample of 58881 people and was published by the Norwegian Institute of Public Health in 2010. In the study, it was found that only 6% of the sample group preferred ce- sarean section to vaginal birth. Factors such as pre- vious cesarean section experience, fear of birth, and negative birth experience affect the choice of cesar- ean section (31).
This study aims to determine the factors affecting the cesarean section attitudes of women aged 18- 49 in the Turkish sample, through scale development. The unique point of this study is that the factors de- termining the attitude towards caesarean section in the Turkish sample were not determined through scale development. When the literature is examined, although there are qualitative and quantitative stu- dies on cesarean section preferences, precautions to be taken to prevent anxiety and depression that develop with cesarean section, and studies on the financial burden that cesarean section brings to the country’s health system, it was determined that a ce- sarean attitude scale that takes a group directly at birth age as a sample is missing. has been made. It is anticipated that this scale will fill an important gap and guide future studies.
![]()
![]()
In this study, permission was obtained from the eth- ics committee of Istanbul Esenyurt University with the decision dated December 1, 2022 and numbered 2022-11/11. While obtaining data within the scope of the study, the principles in the Declaration of Hel- sinki were followed.
Sample included women in reproductive age be- tween 18-49 years residing in Esenyurt district of Istanbul/Turkey province. In the study, 437 women were reached using convenience sampling. When the literature is examined, it is seen that there are differ- ent opinions about sample size in scale development studies. The number of participants to be reached should be 5 times, and if possible 10 times, the num- ber of statements (32-33). Hinkin (1995) argues that 4 to 10 times as many individuals as the scale items will be sufficient (34). While Kline (1994) stated that at least 100 people are sufficient for scale develop- ment studies (35), Gorsuch (2014) determined this number ranges from 50 to 200 (36). This informa- tion adequately represents the liberation of 437 in- dividuals for the scale consisting of 20 items, and the universe within the framework of these views. De- mographic information of the women included in the study (age, reproductive status, childbearing status, etc.) were not considered.
The conceptual framework of the research discusses the structural relationships between the factors (al- ternative choice, preference, negative effect, facili- tating attitude and special choice) that are effective in the caesarean section attitude, which are the main variables of the research.
Explanations regarding the scale sub-dimensions that emerged after the conceptual model are as follows;
Alternative Choice: In cases where normal birth is im- possible and the excessive pain is present, the birth preference is cesarean section.
Preference: It is the factor that expresses the indi- vidual’s preference for cesarean section even if there is a possibility of normal birth.
Negative Effect: Dimension that expresses that ce- sarean section is a negative situation for the mother, baby and family.
Facilitative Attitude: It states that cesarean section is simpler and more comfortable than vaginal birth.
Special Choice: The individual’s body aesthetics is the dimension that expresses the individual’s choice of cesarean section so that the child is born on an important day for him/her and/or his/her partner.
Negative Effect: This is the dimension that express- es that cesarean section is a negative situation for the mother, baby and family.
The data were collected by face-to-face survey meth- od between 1 January 2023 and 30 July 2023. While preparing the survey of the research, the conceptual framework was created based on the literature (17, 27-31). In accordance with this conceptual structure, the question pool was created by the researchers.
![]()
![]()
Firstly, the conceptual framework for the scale to be developed was created by reviewing the relevant literature. In the next stage, an item pool consist- ing of 42 questions was developed. Following this stage, the opinions of 10 experts (CVI: 0.62) who serve as faculty members in the faculties of health sciences (4 people), educational sciences (2 people), and business sciences (4 people) of universities in Turkey were consulted using the Lawshe technique. After the expert opinions, the number of questions in the pool was reduced to 32. The content validity of the remaining 32 questions was found to be 84%. A pilot study was conducted on a group of 20 people, so that errors in the items such as expression errors,
misunderstanding by the respondents, spelling er- rors, spelling mistakes, etc. were corrected. For test- retest reliability, the draft scale was administered to 25 people twice at 3-week intervals and the total scores obtained from the scale are given below. The level (degree) of Pearson correlation coefficient be- tween the first and second application is 0.82 (82%). There is a very strong (very high) positive correlation between the first and second application. That is to say, the measurements made at different times are very similar. Therefore, the scale is highly reliable. Fi- nally, the survey was administered to a target group of 437 people.
Reliability analysis was performed on the data ob- tained from the target group using “item analysis based on item-total correlation” and the reliability coefficient for the remaining 20 statements in the final scale was found to be α= 0.820. Since this value is between 0.80≤α<1.00, the scale is highly reliable. In addition, for the sub-factors of the scale, namely Alternative Choice Factor, Preference Factor, Nega- tive Impact Factor and Facilitating Attitude Factor, 0,80≤α<1,00 is valid and the factors are highly re- liable. For the Special Choice Factor, 0,60≤α<0,80 is valid. This indicates that the factor is reliable.
An explanatory factor analysis was conducted for the data. In the analysis, the items (7, 8, 9, 14, 15,
16, 17, 18, 19, 27, 30, 31) that did not fit were re- moved from the scale and the results in Table 1 were obtained.
Since the Keiser Meyer Olkin Test (KMO) value is 0.844, the result is excellent. The high KMO value indicates that the sample size is sufficient for factor analysis. The result of Bartlett’s test is also signifi- cant (p<0,05). In other words, there are high correla- tions between the variables and the data come from Multivariate Normal Distribution (42). In accordance with both findings, the data are suitable for factor analysis and the sample is sufficient. A factor loading value above 0.30 is sufficient. The smallest factor loading value of the analysis was found to be 0.448. The cumulative variance explained by the eigenval- ues is 67.35% of the total variance.
As a result of the analyses of the items whose rotat- ed (rotation type: Varimax) factor loadings were cal- culated, it is seen that the scale consists of 20 items and 5 dimensions. While determining the factor load- ings as a result of the explanatory factor analysis, care was taken to ensure that the factor loading of
each statement was at least 0.30 and above (Table 1 can be examined for detailed information). Addi- tionally, there are at least 3 statements under each dimension. The dimensions obtained by taking into account the meaning of the items in the factors by utilising the rotated factor loadings were named as “Alternative Choice Factor, Preference Factor, Nega- tive Impact Factor, Facilitating Attitude Factor and Special Choice Factor” respectively.
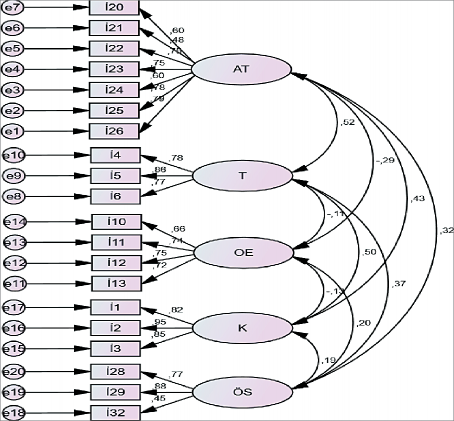
In this section, confirmatory factor analysis (CFA) was applied to the factors affecting the attitude towards caesarean section through IBM AMOS package pro- gramme and the degree of fit of the data for the as- sumed model was tested. Confirmatory factor analy- sis and structural validity analysis were performed, and the diagram of model fit is given in Figure 1.
Acceptable values of the fit indices are χ2/df <5, GFI
>0.85, AGFI >0.90, CFI >0.90, RMSEA <0.08 and RMR
<0.08 (37-39).
The adaptive values given in Table 2 show that the model fit is good. The good fit of the data for the model shows that the model has construct validity.
The results of confirmatory factor analysis (CFA) of the optimised measurement model are as shown in Table 3.
Regression values show the power of observed vari- ables to predict latent variables, i.e. factor loadings. Since the “p” values for each binary relationship above are less than 0.001, the factor loadings are significant. The significant p values indicate that the items are loaded correctly on the factors. In addition, standardised regression coefficients of 0.452 and above indicate that the ability to predict latent vari- ables, i.e. the factor loadings of each item are high.
Even if the AVE value is less than 0.50, the conver- gent validity is ensured when the CR is greater than
0.60 (40). Since the AVE values calculated in the table above are 0.52 and above and the CR value is 0.62 and above, the model provides convergence validity.
Table 1. Results of the explanatory factor analysis of the study
Factor
Variables
I21: If I had pelvic stenosis (narrowness of the birth canal) for birth, I would definitely prefer a cesarean delivery.
.669
I23: During my pregnancy, if the doctor told me that my baby was a big baby, I would definitely prefer a cesarean delivery.
.813
I25: Since I don’t think I will be able to push for a long time during birth, I definitely prefer a cesarean section.
.589
oadings Explained
Factor Variance
L
I20: I prefer a cesarean section because I am very afraid of vaginal birth. .468
I22: If I had a twin pregnancy, I would definitely prefer a cesarean delivery. .784
Alternative
Choice
I24: If the process did not progress during birth, I would definitely prefer a cesarean section to avoid any trouble.
.769
29.761
I26: Since I do not want to suffer pain for a long time during birth, I definitely prefer cesarean delivery.
.601
Preference
I4: In any case, I would like to give birth by cesarean section. .728
I5: I would like to give birth by cesarean section, whether my doctor recommends .853
it or not.
14.138
Negative Impact
I5: I would like to give birth by cesarean section, whether my wife and family want it or not.
I10: Caesarean section negatively affects communication between mother and baby.
.796
.770
I11: Caesarean section negatively affects women’s life for life. ,783
9.292
I12: Caesarean section negatively affects communication between spouses. ,821
I13: Caesarean section negatively affects the mother’s breastfeeding. .774
Facilitating Attitude
I1: Cesarean section is usually easier than vaginal birth method. .862
I2: Cesarean section is generally easier than vaginal birth method. .899
I3: Cesarean section is usually more comfortable than vaginal birth method. .833
8.143
Special Choice
I28: I would definitely prefer a cesarean section to give birth to my baby on a special date for me.

Evaluation Criteria
Kaiser-Meyer-Olkin Measure of Sampling Adequacy: 0.844 Approx. Chi-Square: 4249.725
Barlett’s Test of Sphericity: 0.000 Cronbach Alpha’s: 0.820
Extraction Method: Principal Components Rotation Method: Varimax Total Variance Explained: 67.350
I29: I prefer cesarean section because I consider my body aesthetics after birth. .861
I32: If my doctor recommended a cesarean birth, I would prefer a cesarean birth without hesitation.
.828
.627
6.018
Table 2. Results of the model fit of the study | |
Acceptable Fit Indices | Calculated Fit Indices |
CMIN/df (χ2/sd) | 3.451 |
GFI | 0.876 |
IFI | 0.906 |
CFI | 0.905 |
RMSEA | 0.077 |
SRMR | 0.0612 |
![]()
![]()
Figure 1. Results of measurement model and goodness of fit
Table 3. The results of confirmatory factor analysis for the optimised measurement model | |||||||||
Factors | Statement | Standardised Value | Estimate | Standard Value | T value | p | Cronbach’s α | AVE | CR |
I20 | .597 | .777 | .062 | 12.476 | *** | ||||
I21 | .477 | .576 | .059 | 9.743 | *** | ||||
I22 | .749 | .923 | .057 | 16.231 | *** | ||||
Alternative Choice | I23 | .749 | .932 | .057 | 16.219 | *** | |||
I24 | .595 | .741 | .060 | 12.437 | *** | 0.857 | .50 | .79 | |
I25 | .778 | .932 | .055 | 16.967 | *** | ||||
I26 | .794 | 1.000 | *** | ||||||
I4 | .785 | 1.046 | .065 | 16.091 | *** | ||||
Preference | I5 | .855 | 1.072 | .063 | 17.050 | *** | 0.841 | .65 | .76 |
I6 | .774 | 1.000 | *** | ||||||
I10 | .663 | .965 | .080 | 12.043 | *** | ||||
Negative Impact | I11 | .742 | 1.076 | .082 | 13.189 | *** | |||
I12 | .749 | 1.040 | .078 | 13267 | *** | 0.810 | .52 | .73 | |
I13 | .723 | 1.000 | *** | ||||||
I1 | .820 | 1.037 | .049 | 21.032 | *** | ||||
Facilitating Attitude | I2 | .946 | 1.110 | .045 | 24.584 | *** | 0.900 | .76 | .83 |
I3 | .846 | 1.000 | *** | ||||||
I28 | .769 | 1.538 | .177 | 8.706 | *** | ||||
Special Choice | I29 | .875 | 1.714 | .201 | 8.527 | *** | 0.714 | 0.52 | .62 |
I32 | .452 | 1.000 | *** | ||||||
![]()
![]()
Although there is no study on the development of a direct psychometric measurement tool related to cesarean section in the Turkish sample, it is possible to say that there is literature on this field. Antoine and Young (2021), Opiyo (2022), Torloni et al. (2011) reported that cesarean section has a negative ef- fect (19-21) on both mother and child health, which is like the “negative impact” sub-factor of the scale developed within the scope of this study. Liang et al. (30) when the findings of the study introduced to the field are examined, among the factors affecting the choice of cesarean section is the desire for the baby to be born on a special day for the family. This finding is similar to the “Special Choice” factor, which is one of the sub-dimensions of the scale developed within the scope of this study. When the literature is examined, there are findings that individuals are di- rected to cesarean section, especially by physicians, and their preference for cesarean section is due to fear of birth (2-5). These findings are like the prefer- ence factor of the measurement tool introduced to the field within the scope of this study. When the literature is examined, there are findings (6,9,31) that the individual must choose cesarean section as an alternative in cases where normal birth is not pos- sible. These findings are like the alternative prefer- ence factor, which is one of the sub-dimensions of this study. Situations such as the individual’s previ- ous miscarriage or fear of childbirth are explained by the facilitating attitude factor, which is one of the sub-dimensions within the scope of this study. This factor is like studies in literature (1,28-29).
![]()
![]()
In this study, a valid and reliable measurement tool was developed that includes all stages of the scale development process (41-43) in the literature. The developed scale consists of 5 factors and 20 state- ments (alternative choice factor - 7 items, preference factor - 3 items, negative impact factor - 4 items,
facilitating attitude factor - 3 items, special choice factor - 3 items). The developed measurement tool can be used to determine the attitudes of women of childbearing age and adulthood towards cesarean section in the Turkish sample. It is anticipated that this study will guide future studies.
![]()
![]()
Özkan S, Aksakal F, Avcı E, Civil EF, Tunca MZ. Kadın- ların doğum yöntemi tercihi ve ilişkili faktörler. Turk J Public Health. 2013;11(2):59-71. Turkish.
Karabulutlu Ö. Kadınların doğum şekli tercihleri- ni etkileyen faktörler. Florence Nightingale J Nurs. 2012;20(3):210-8. Turkish.
Ergöl Ş, Kürtüncü M. Bir üniversite hastanesinde ka- dınların sezaryen doğum tercihlerini etkileyen faktör- ler. Hacettepe Üniversitesi Hemşirelik Fakültesi Dergi- si. 2014;1(3):26-34. Turkish.
Uçar T, Gölbaşı Z. Nedenleri ve sonuçlarıyla do- ğum korkusu. Annals of Health Sciences Research. 2015;4(2):54-8. Turkish.
Ryding EL, Lukasse M, Parys ASV, Wangel AM, Karro H, Kristjansdottir H, et al. Fear of childbirth and risk of cesarean delivery: a cohort study in six European countries. Birth. 2015;42(1):48-55.
Larsson B, Karlström A, Rubertsson C, Hildingsson I. The effects of counseling on fear of childbirth. Acta Obstet Gynecol Scand. 2015;94(6):629-36. https:// doi.org/10.1111/aogs.12634.
Terzioğlu F, Gençbaş D, Boztepe H, Doğu N, Akdeniz C, Yüceer B. Sezaryen Sonrası Kaygı ve Depresyon: Non-Farmakolojik Kanıt Temelli Uygulamalar. Dokuz Eylül Üniversitesi Hemşirelik Fakültesi Elektronik Der- gisi. 2022;15(3):395-401. https://doi.org/10.46483/ deuhfed.790640. Turkish.
Vural G, Şentürk Erenel A. Doğumun Medikalizasyonu Neden Artmıştır, Azalta Bilir Miyiz? Hacettepe Üniver- sitesi Hemşirelik Fakültesi Dergisi. 2017;4(2):76-83. Turkish.
Çakmak B, Arslan S, Nacar M. Kadınların isteğe bağlı sezaryen konusundaki görüşleri. Fırat Tıp Dergisi. 2014;19(3):122-5. Turkish.
Altuntaş H, Dansuk R, Köse O. Sezaryen oranlarının çe- şitli değişkenlere bağlı olarak değerlendirilmesi. Kırık- kale Üniversitesi Tıp Fakültesi Dergisi. 2013;15(2):1-
7. Turkish.
Güven Ay G, Taşçı Duran E. Sezaryen Yöntemi ile Do- ğum Yapan Kadınların Sezaryen Sonrası Vajinal Doğu- ma Bakış Açılarının İncelenmesi. Journal of Ege Univer- sity Nursing Faculty. 2022;38(3):183-92. https://doi. org/10.53490/egehemsire.1081072. Turkish.
Hofmeyr JG, Novikova N, Mathai M, Shah A. Techniques for cesarean section. Am J Obstet Gynecol. 2009;201(5):431-
4. https://doi.org/10.1016/j.ajog.2009.03.018.
Veef E, Van de Velde M. Post-cesarean section analge- sia. Best Pract Res Clin Anaesthesiol. 2022;36(1):83-
8. https://doi.org/10.1016/j.bpa.2022.02.006.
Harrison MS, Goldenberg RL. Cesarean section in su- b-Saharan Africa. Mater health neonatol perinatol. 2016;2:1-10. https://doi.org/10.1186/s40748-016-
0033-x.
Sewell JE. Cesarean section–a brief history. A brochure to accompany an exhibition on the history of cesarean section at the National Library of Medicine; 1993.
Gündoğdu G. In-Bed Exercises After Cesarean Section, Early Oral Hydration and Effect of Gum Chewing on Bowel Movements, Pain and Breastfeeding [Doctoral Thesis]. Atatürk University Institute of Health Scien- ces; 2019. Turkish.
Mylonas I, Friese K. Indications for and risks of electi- ve cesarean section. Dtsch Arztebl Int. 2015;112(29- 30):489-9. https://doi.org/10.3238/arztebl.2015.0489.
Coutinho IC, de Amorim MMR, Katz L, de Ferraz ÁAB. Uterine exteriorization compared with in situ repa- ir at cesarean delivery: a randomized controlled tri- al. Obstet Gynecol. 2008;111(3):639-47. https://doi. org/10.1097/AOG.0b013e31816521e2.
Antoine C, Young BK. Cesarean section one hund- red years 1920–2020: the Good, the Bad and the Ugly. J Perinat Med. 2021;49(1):5-16. https://doi. org/10.1515/jpm-2020-0305.
Opiyo N, Torloni MR, Robson M, Ladfors L, Gholbzouri K, Kacerauskiene J, et al. WHO’s Robson platform for data-sharing on caesarean section rates. Bull Wor- ld Health Organ. 2022;100(5):352-4. https://doi. org/10.2471/BLT.21.287742.
Torloni MR, Betran AP, Souza JP, Widmer M, Allen T, Gulmezoglu M, et al. Classifications for cesarean secti- on: a systematic review. PloS One. 2011;6(1):e14566. https://doi.org/10.1371/journal.pone.0014566.
Füsun A, İğde A. Normal Vaginal Birth After Cesarean Section. Contin Med Educ. 2004;13:137-9.
Çağlayan EK, Kara M, Gürel YC. Evaluation of risk factors and potential complications after cesarean operations in our clinic. Med J Bakirkoy. 2011;7(2):64-
67. doi:10.5350/BTDMJB201107205. Turkish.
Kurt Can E, Ejder Apay S. Mode of Delivery: Does it Affect Postpartum Comfort and Birth Satisfaction Levels? Journal of İnönü University Vocational Scho- ol of Health Services. 2020;8(3):547-65. https://doi. org/10.33715/inonusaglik.753497. Turkish.
Demirbaş M, Karabel MP, İnci MB. Changing cesarean section frequency and possible causes in Turkey and in the world. Sakarya Medical Journal. 2018;7(4):158-
63. Turkish.
Yeşilçiçek Çalık K, Erkaya R, Karabulutlu Ö. Rates and Indications of 4-Year Cesarean Delivery in a Tertiary Hospital. Arch Health Sci Res 2018;5:201-9.
Akdolun Balkaya N, Vural Ş, Eroğlu K. Investigating Problems Related to The Health of Mothers and Their
Babies Resulting From Risk Factors Determined Du- ring Pregnancy. J DU Health Sci Inst. 2014;4(1):6-16. Turkish
Perner MS, Ortigoza A, Trotta A, Yamada G, Bronstein AB, Friche AA, et al. Cesarean sections and social inequ- alities in 305 cities of Latin America. SSM-population health. 2022;19:101239. https://doi.org/10.1016/j. ssmph.2022.101239.
Okyere J, Duah HO, Seidu AA, Ahinkorah BO, Budu E. Inequalities in prevalence of birth by caesarean sec- tion in Ghana from 1998-2014. BMC Pregnancy and Childbirth. 2022;22(1):64. https://doi.org/10.1186/ s12884-022-04378-8.
Liang H, Fan Y, Zhang N, Chongsuvivatwong V, Wang Q, Gong J, et al. Women’s cesarean section preferences and influencing factors in relation to China’s two-child policy: a cross-sectional study. Patient Prefer Adhe- rence. 2018;12:2093–101.
Fuglenes D, Aas E, Botten G, Øian P, Kristiansen IS. Why do some pregnant women prefer cesarean? The influence of parity, delivery experiences, and fear. Am J Obstet Gynecol. 2011;205(1):45-e1. https://doi. org/10.1016/j.ajog.2011.03.043.
Nunnally J. Psychometric Theory, 3rd ed. New York: McGraw-Hill; 1994.
Bryman A, Cramer D. Quantitative Data Analysis with SPSS Release 10 for Windows. Routledge; 2001. https://doi.org/10.4324/9780203471548
Hinkin TR. A review of scale development practices in the study of organizations. J manag. 1995;21(5):967-
88. https://doi.org/10.1177/014920639502100509.
Kline P. An easy guide to factor analysis. London: Routled- ge; 1994.
Gorsuch RL. Factor analysis (Classic edition). New York: Routledge; 2014. https://doi.org/10.4324/ 9781315735740.
Munro BH. Statistical methods for health care resear- ch (Vol. 1). Lippincott Williams & Wilkins; 2005.
Hooper D, Coughlan J, Mullen MR. Structural equa- tion modelling: Guidelines for determining model fit. Electron J Bus Res Methods. 2008;6(1):53-60.
Schumacher RE, Lomax RG. A beginners guide to structural equation modeling: SEM. New Jersey: Lawrence Erlbaum Associates; 2010.
Hair JJF, Black WC, Babin BC, Anderson RE. Multivariate Data Analysis. International Encyclopedia of Statisti- cal Science. Berlin: Springer Heidelberg; 2010. https:// doi.org/10.1007/978-3-642-04898-2_395
DeVellis F.Ölçek Geliştirme Kuram ve Uygulamalar (Scale Development Theory and Applications), Çev. Ed: Totan, T. Ankara: Nobel Akademik Yayıncılık. 2022.
3. Basım. Turkish.
Karagöz Y. SPSS ve AMOS uygulamalı nitel-nicel-kar- ma bilimsel araştırma yöntemleri ve yayın etiği. Anka- ra: Nobel Akademik Yayıncılık; 2021. Turkish.
Karagöz Y, Bardakçı S, Bilimsel Araştırmalarda Kullanılan Ölçme Araçları ve Ölçek Geliştirme. Ankara: Nobel aka- demik yayıncılık; 2020. Turkish.
![]()
![]()
![]()
![]()
Uvod. Carski rez alternativa je normalnom porodu i izvodi se kroz rez. Carski rez može biti metoda koja se primjenjuje u slučajevima nužde, ali se može primije- niti i u slučajevima kada nije obvezan.
Cilj. Cilj je ovog istraživanja utvrditi stavove žena pre- ma carskom rezu.
Metode. U istraživanje je bilo uključeno 437 žena reproduktivne dobi, u dobi od 18 do 49 godina koje žive u okrugu Esenyurt u pokrajini Istanbul. Prvo je sastavljena anketa od 42 pitanja. Nakon dobivenoga stručnog mišljenja i provođenja pilot-studije, nacrt ankete koji se sastojao od 32 pitanja primijenjen je u istraživanju. Prvi korak u analizi podataka bila je ek- sploratorna faktorska analiza. Nakon analize, iz ska- le je uklonjeno 12 pitanja koja se nisu svrstala ni u jedan faktor, a utvrđena je struktura od pet faktora koja sadržava 20 pitanja. Potom je provedena konfir- matorna faktorska analiza.
Rezultati. Utvrđeno je da dobiveni model savršeno odgovara podacima. Stoga je skala razvijena eksplo- rativnom faktorskom analizom potvrđena konfirma- tornom faktorskom analizom. Cronbachov koeficijent razvijene skale iznosi 0,820 te je zaključeno da je skala vrlo pouzdana.
![]()
Zaključak. Zaključeno je da se razvijena skala može upotrebljavati za mjerenje stavova žena prema car- skom rezu.
Ključne riječi: carski rez, skala stavova, razvoj skale, Turska
![]()