
![]()
![]()
![]()
1 Saliha Koç Aslan
1 Acibadem Health Group Head Office Ataşehir, Istanbul
![]()
Article received: 14. 08. 2025.
![]()
Article accepted: 10. 12. 2025.
![]()
https://doi.org/10.24141/2/10/1/5
![]()
Author for correspondence:
Saliha Koç Aslan
Acibadem Health Group Head Office Ataşehir, Istanbul E-mail: skoc@acibadem.com
![]()
Keywords: behavioral model, leadership competencies, nurse managers, personality assessment, DISC model
![]()
![]()
![]()
![]()
![]()
Effective nursing management and leadership play a critical role in shaping patient outcomes, improving staff well-being, and supporting the operational effi- ciency of healthcare organisations. Nurse managers— particularly those in middle and senior leadership roles—serve as essential intermediaries between clinical practice and administrative decision-making. Understanding their behavioural tendencies is there- fore crucial for cultivating work environments that enhance staff satisfaction, organisational communi- cation, and patient safety (1–6).
The Dominance–Influence–Steadiness–Conscientious- ness (DISC) behavioural model, developed by William Moulton Marston in the 1920s, categorises behav- ioural tendencies into four domains: Dominance (D), Influence (I), Steadiness (S), and Conscientiousness
(C) (7–10). Widely used in organisational psychology, the DISC model supports improvements in leader- ship effectiveness, interpersonal communication, and team functioning (7). In healthcare settings, aligning leadership responsibilities with behavioural strengths may reduce job stress, improve efficiency, and increase job satisfaction—particularly in high- pressure environments such as hospitals (11).
Conscientiousness—characterised by accuracy, reli- ability, and attention to detail—is especially impor- tant in nursing leadership, where accountability and precision are essential (12–14). Leaders who demonstrate conscientious behavioural tendencies often contribute to cultures of safety and quality, positively affecting team performance and patient outcomes (4). Interpersonal traits such as Influence also support leadership effectiveness by enhancing motivation, engagement, and communication within teams (11,13,15).
Personality assessments, including the DISC model, are increasingly used to inform leadership develop- ment initiatives. Targeted educational programmes can be designed around the behavioural patterns of nurse leaders, enabling organisations to strengthen decision-making, communication, and motivational competencies (16). For example, individuals with high Steadiness may benefit from training in rapid decision-making under pressure (12). Additionally, linking personality traits with transformational or
transactional leadership styles may help organisa- tions identify and develop individuals best suited for leadership roles (11,12,17,18).
Personality traits also influence ethical leadership behaviours, which play a vital role in shaping or- ganisational culture, employee morale, and retention (13,19). Ethical, consistent leadership strengthens trust and contributes to a positive work climate, re- inforcing the importance of understanding leaders’ behavioural patterns (4,20,21).
Understanding the full spectrum of DISC behavioural profiles—not only conscientiousness—provides valua- ble insight into how different personality tendencies align with the characteristics required for effective leadership in healthcare settings (7–9,22). Previous research demonstrates that personality assessments such as the DISC model can effectively identify an individual’s strengths, developmental needs, and op- timal areas of contribution, enabling organisations to deploy leaders in ways that maximise their impact within teams (23–26).
Despite growing international interest in behavioural leadership assessments, limited research has exam- ined DISC behavioural tendencies among nurse lead- ers in Türkiye. Understanding the distribution of DISC profiles in this population is essential for designing effective leadership development strategies tailored to local healthcare contexts. Identifying behavioural strengths and limitations can also support competen- cy planning, workforce development, and improve- ments in organisational leadership structures.
This study provides the first comprehensive ex- amination of DISC behavioural tendencies among mid- and senior-level nurse managers in Türkiye. By linking DISC profiles with behavioural, communica- tion, decision-making, managerial, and motivational competencies, the study offers new insights into leadership patterns within Turkish nursing manage- ment. These findings inform future leadership devel- opment programmes and contribute to the limited body of evidence on behavioural leadership models in Turkish healthcare settings.
![]()
![]()
This study aimed to:
Identify the dominant DISC behavioural char- acteristics of nurses in mid-level and senior management roles.
Evaluate their behavioural, communication, decision-making, managerial, and motivational competencies, and explore how these align with their DISC profiles.
![]()
![]()
This descriptive cross-sectional study was conducted between 1 and 31 May 2021 within a large private healthcare group in Türkiye, comprising 16 hospitals and 4 medical centres. The Dominance–Influence– Steadiness–Conscientiousness (DISC) behavioural assessment is routinely administered in this insti- tution as part of its annual leadership development programme for Nurses in Charge, Nurse Managers, and Nurse Educators. The study was carried out dur- ing the COVID-19 pandemic, a contextual factor that may have influenced managerial workload, stress levels, and leadership behaviours.
The target population included all middle- and senior- level nurse managers employed in the participating facilities during the study period. Due to the limited size of the managerial workforce and the exploratory nature of the study, no formal sample size calculation was conducted. Instead, a census sampling approach was used, inviting all 280 eligible managers to par- ticipate. A total of 186 managers completed the sur- vey, yielding a response rate of 66.4%.
The inclusion criteria were:
Employment in a middle or senior nursing man- agement role (e.g., Nurse in Charge, Depart- ment Manager).
A minimum of one year of experience in a leadership position.
The exclusion criteria were:
Acting leadership roles of less than six months.
Extended leave during the study period.
The primary variable of interest was the distribution of DISC behavioural profile types—Dominance, Influ- ence, Steadiness, and Conscientiousness. Predictor variables included age, gender, education level, pro- fessional nursing experience, managerial experience, and prior leadership training.
Based on existing research and institutional obser- vations, it was hypothesised that Conscientiousness would be the most common dominant DISC style among nurse leaders and that associated leadership competencies would reflect systematic, collabora- tive, and evidence-based behaviours.
DISC Behavioral Assessment
The DISC Behavioral Assessment used in this study is a standardised and licensed psychometric instrument consisting of 28–40 forced-choice items that evaluate behavioural preferences across four major domains:
Dominance (D): assertiveness, decisiveness, competitive orientation
Influence (I): sociability, enthusiasm, persuasion
Steadiness (S): patience, empathy, cooperation
Conscientiousness (C): accuracy, analytical thinking, structured work style
Instrument details (added per statistical reviewer requirements):
Version: DISC Classic 2.0 (institutional licensed version)
Publisher: PeopleKeys® / DISCinsights®
Language: Turkish professionally translated version
Scoring method: Ipsative forced-choice scoring generating dominant and secondary profiles
License: Used under institutional leadership development authorization
The DISC model is widely validated internationally, with published Cronbach alpha coefficients typically ranging from 0.72–0.87 across behavioural domains. However, due to the ipsative scoring structure, in- ternal consistency measures (e.g., Cronbach’s alpha) cannot be meaningfully calculated for this dataset, which aligns with psychometric standards for forced- choice assessments.
Competency Mapping Questionnaire
A structured 40-item competency questionnaire de- veloped by the institution’s Nursing Services Direc- torate was used to evaluate leadership competen- cies in five domains:
Behavioural Competencies: Extroversion, indi- viduality, entrepreneurship, positive thinking, logical prioritisation, adaptability, rule adher- ence, quality orientation, systematic planning, guidance and support, risk aversion, and sta- bility maintenance.
Communication Competencies: Evidence-based communication, active listening, persuasive ability, audience engagement, and maintaining conversational relevance.
Decision-Making Competencies: Data-based anal- ysis, independent judgment, system-aligned de- cision-making, optimal option selection, and rapid decision-making under pressure.
Management Competencies: Strategic vision, initiative, authority establishment, stress man- agement, calculated risk-taking, innovation adoption, long-term planning, teaching-based delegation, work discipline, team motivation, inspiring leadership, and empathy.
Motivation Style Competencies: career planning, provision of social support, creation of a positive environment, and fostering team inclusion.
The tool reflects organisational competency expec- tations for nurse leaders, though it does not have published psychometric validation—an issue acknowl- edged as a limitation.
Data were collected through a secure online platform and included:
The standardised DISC Assessment
The institutional competency questionnaire
Recruitment and Administration
Invitations were distributed electronically through official institutional channels.
Participation was voluntary, and informed con- sent was obtained electronically.
No identifiable personal data were collected.
All participants completed the DISC application under standardised institutional conditions.
Bias Reduction Measures
Use of a validated, standardised DISC tool
Uniform administration procedures across all facilities
Census recruitment to minimise selection bias
Predefined data analysis plan to avoid selec- tive reporting
The online format enabled participation from man- agers across all 4 medical centres and 16 hospitals, ensuring broad representation.
The study adhered to the ethical principles of the Declaration of Helsinki-2013 (27). Although formal ethics committee approval was not required due to the institution’s internal assessment policies, several ethical safeguards were implemented:
Written informed consent was obtained from all participants.
Institutional approval was secured for conduct- ing the study and disseminating the findings.
All data were anonymised and stored confi- dentially.
Participants were informed of their right to withdraw at any stage without penalty.
These measures ensured that participant rights, pri- vacy, and welfare were upheld throughout the re- search process.
Due to the descriptive and exploratory nature of the research, statistical analyses were limited to frequen- cies, percentages, means, and standard deviations. Although inferential statistics are referenced in some literature, they were not used in this study; interpreta- tions rely strictly on descriptive findings. SPSS v25 was used. A sensitivity analysis excluding incomplete DISC results confirmed that findings remained unchanged.
![]()
![]()
Table 1 summarises the socio-demographic charac- teristics of the participating nurse leaders. The ma- jority of respondents were female (75.3%), and most held undergraduate (38.7%) or postgraduate degrees (21.5%). The workforce was highly experienced, with 78.5% reporting more than 61 months of professional experience. In terms of departmental distribution, nearly half worked in inpatient units (43.0%), followed by Nurse Specialist roles (18.8%) and outpatient ser- vices (13.4%). Most participants held the position of Nurse in Charge (81.2%), indicating strong representa- tion from frontline leadership roles.
The average age of participants was 37.13 years (range: 27–48 years), reflecting a mature and expe- rienced leadership cohort.
Table 1. The Socio-Demographic Characteristics of The Nurses | ||
Gender | n | % |
Female | 140 | 75.3 |
Male | 46 | 24.7 |
Education | n | % |
High School | 58 | 31.2 |
Associate degree | 16 | 8.6 |
Undergraduate | 72 | 38.7 |
Postgraduate | 40 | 21.5 |
Work Experience | n | % |
0-12 Months | 7 | 3.8 |
13-36 Months | 16 | 8.6 |
37-60 Months | 17 | 9.1 |
61 Months and Over | 146 | 78.5 |
Department | n | % |
Inpatients | 80 | 43.0 |
Nurse Specialist | 35 | 18.8 |
Outpatients | 25 | 13.4 |
Intensive Care Units | 16 | 8.6 |
Emergency Services | 12 | 6.5 |
Operating Room | 10 | 5.4 |
Position | n | % |
Nurse in Charge | 151 | 81.2 |
Education and Development Nurse | 18 | 9.7 |
Manager | 17 | 9.1 |
Total | 186 | 100.0 |
Table 2 presents the distribution of dominant DISC behavioural traits across the 186 participating nurse leaders. Conscientiousness (C) was the most preva- lent dominant trait overall, reported by 54.8% of the sample. This pattern was especially pronounced among Nurses in Charge, 45.6% of whom demon- strated a primarily conscientious profile. Managers also showed a notable inclination toward conscien- tiousness (5.37%).
Influence (I) emerged as the second most common trait, particularly among Nurses in Charge (12.8%) and Education and Development Nurses (3.76%). Steadiness (S) and Dominance (D) were comparative- ly less frequent across all leadership groups. Overall, Conscientiousness remained the consistently domi- nant behavioural style across all managerial posi- tions (Table 2).
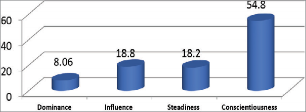
Graphic 1. DISC Personality Distribution of Nurses
Table 3 presents the distribution of general behav- ioural characteristics among the participants. Most traits—such as efficiency orientation, assertiveness, charisma, persistence, friendliness, precision, and consideration—clustered predominantly within the normal range, indicating generally balanced behav- ioural patterns among nurse leaders.
A notable exception was independence, where 44.6% of participants scored very low, suggesting a preference for collaborative or system-dependent working styles. Patience and tolerance demonstrated predominantly high levels, while sharing emerged as an exceptionally strong trait, with 44.6% of respond- ents scoring very high.
Self-motivation showed a downward tendency, with 37.6% of participants reporting low levels. Observa- tion and awareness were distributed mainly within the normal range, though a meaningful proportion achieved high scores.
Overall, the findings suggest a largely well-balanced behavioural profile among nursing leaders, while highlighting distinct tendencies in areas such as in-
Table 2. DISC Personality Distribution of Nurses | ||||
The Most Dominant Factor | Manager | Nurse in Charge | Educational Development Nurse | Total |
n % | n % | n % | n % | |
Dominance (D) | 1 | 0.53 | 10 | 5.37 | 4 | 2.14 | 15 | 8.06 |
Influence (I) | 4 | 2.14 | 24 | 12.8 | 7 | 3.76 | 35 | 18.8 |
Steadiness (S) | 2 | 1.07 | 32 | 17.1 | 0 | 0 | 34 | 18.2 |
Conscientiousness (C) | 10 | 5.37 | 85 | 45.6 | 7 | 3.76 | 102 | 54.8 |
Total | 17 | 9.1 | 151 | 81.1 | 18 | 9.6 | 186 | 100.0 |
Table 3. The General Behavioral Competencies Distribution of Nurses | |||||||
The general behavioral competencies | Very Low n % | Low n % | Normal n % | High n % | Very High n % | Group Average | SS(±) |
Self-Motivation 49 26.3 70 37.6 47 25.2 14 7.5 6 3.23 Low 1.02
Efficiency Orientation
20 10.8 39 21 100 53.8 18 9.7 9 4.8 Normal 0.94
Assertiveness 59 31.7 39 20.9 68 36.6 15 8.06 5 2.7 Normal 1.08
Independence 83 44.6 42 22.6 51 27.4 7 3.7 3 1.6 Very Low 1.009
Persistence 12 6.4 38 20.4 110 59.1 21 11.3 4 2.1 Normal 0.8
Charisma, Impressiveness
41 22.04 50 26.9 65 34.9 23 12.4 7 3.8 Normal 1.08
Patience, Tolerance 7 3.8 14 7.6 46 24.7 63 33.9 56 30.1 High 1.07
Friendliness, Friendship
8 4.3 18 9.7 101 54.3 37 19.9 22 11.8 Normal 0.94
Being Considerate 7 3.8 18 9.7 70 37.6 48 25.8 43 23.1 Normal 1.06
Sharing 3 1.6 7 3.8 48 25.8 45 24.2 83 44.6 Very High 1
![]()
Awareness, Observation
4
2.15 20 10.7 108 58.06 42 22.5 12 6.45
High
1.07
Precision, Attention to Detail
5 2.7 15 8.06 68 36.5 37 19.8 61 32.7 Normal 0.93
dependence, self-motivation, and interpersonal gen- erosity (Table 3).
The evaluation of communication competencies demonstrated substantial variation across different skill areas. Grounding in facts emerged as a notable strength, with 42.4% of participants scoring very high, reflecting a strong reliance on evidence and data in communication. In contrast, competencies related to influence and attracting attention were more evenly distributed, with most respondents scoring within the normal (34.9%) or low (26.8%)
ranges. Speaking by listening similarly showed a predominance of normal scores (38.1%). Maintain- ing relevance presented a balanced distribution, with 36.02% rated as normal and 32.7% rated as very high. Overall, while factual communication is a key strength, other communication competencies—such as influence, attentive listening, and relevance—were more evenly balanced among participants (Table 4).
Decision-making competencies revealed additional patterns. Paying Attention to Data was most frequent- ly rated as normal (36.02%), followed closely by very
high (33.3%). Independent decision-making also fell predominantly within the normal range (38.1%), in- dicating moderate autonomy. Notably, both Decision- Making in Parallel With the System and the Ability to Choose the Best Result showed the strongest per- formance, with 44.6% of respondents rated as very high, suggesting strong alignment with organisational processes and optimal outcome selection. Conversely, Quick Decision-Making Under Pressure showed sub- stantial challenges, with 44.6% of participants scoring very low, indicating difficulty with rapid decisions in high-pressure situations (Table 4).
Motivation style competencies also displayed distinct tendencies. Career planning emerged as the strongest motivational domain, with 44.08% scoring very high. Supporting social opportunities showed a balanced
showed the highest proportion in the normal range (37.6%), suggesting this competency is generally well-developed but with room for enhancement.
In interpersonal and motivational leadership do- mains, Adding Excitement to Work had the highest proportion in the normal category (36.5%). Effective Speaking and Leadership also clustered primarily in the normal range (34.9%). Notably, Establishing an Emotional Bond with the Team demonstrated strong relational leadership capacity, with high (33.8%) and very high (30.6%) scores, indicating a substantial em- phasis on empathy and emotional connection within management practices (Table 5).
distribution, with most respondents scoring normal
(34.9%). Creating a warm and positive environment
demonstrated a pronounced concentration in the nor- mal range (72.5%), indicating this style is widely and consistently used. Finally, ensuring team inclusion showed high engagement, with substantial propor- tions scoring in the high (34.4%) and very high (30.1%) categories, underscoring strong tendencies toward team-oriented motivational behaviours (Table 4).
Table 5 summarises the distribution of management competencies among the participants. Awareness of the Big Picture was strongest in the high category, with 38.1% of respondents demonstrating strong strategic awareness. Taking the Initiative was most commonly rated as normal (42.4%), while Establish- ing Authority showed a pronounced concentration in the normal range (73.1%), indicating consistent but moderate levels of authoritative leadership.
Competencies related to stress and risk showed clear challenges. Combating Stress was predomi- nantly rated as very low (33.3%), and Risk-Taking also demonstrated a strong very low distribution (45.1%), suggesting a cautious approach and a po- tential need for development in resilience and cal- culated risk behaviour.
In contrast, competencies reflecting forward planning and organisational discipline were notably strong. Be- ing Open to Innovation was most frequently rated as high (38.1%), and Long-Term Strategic Planning and Business Discipline both had the highest concentra- tion in the very high category (44.08%), indicating a strong strategic orientation and structured work ap- proach among nurse leaders. Delegating by Teaching
![]()
This study aimed to identify the dominant DISC be- havioural tendencies of mid- and senior-level nurse leaders and examine how these traits relate to key leadership competencies. The findings revealed a mature and experienced nursing leadership cohort, predominantly female, with strong educational back- grounds and extensive professional and managerial experience. Such a profile aligns with previous re- search highlighting the association between leader- ship self-efficacy, a positive work environment, and readiness to assume formal leadership responsibili- ties (28). This suggests that the organisational con- text provides a suitable foundation for leadership capacity development.
The predominance of Conscientiousness (C) across leadership roles is consistent with the literature de- scribing this trait as essential for nursing manage- ment, given its strong association with accuracy, accountability, and systematic work habits (28). Conscientious leaders are known to support safety culture, structured decision-making, and quality performance—elements that are critical in complex healthcare environments. The presence of Influ- ence (I) as the second most common trait indicates the value of interpersonal and motivational behav- iours, which are central to leadership approaches such as transformational leadership (2,13,29–31). In contrast, lower representation of Steadiness (S) and Dominance (D) reflects a less confrontational and
Table 4. Communication, The Decision-Making, and The Motivation Style Competencies Distribution of Nurses | |||||||
Communication Competencies | Very Low | Low | Normal | High | Very High | ||
n % | n % | n % | n % | n % | Mod | SS(±) | |
Grounding in Facts 9 | 4.8 | 11 | 5.9 | 52 | 27.9 | 35 | 18.8 | 79 | 42.4 | Very High | 1.17 |
Influence, Attract 40 | 21.5 | 50 | 26.8 | 65 | 34.9 | 23 | 12.3 | 8 | 4.3 | Normal | 1.09 |
Speaking by Listening 8 | 4.3 | 18 | 9.6 | 71 | 38.1 | 47 | 25.2 | 42 | 22.5 | Normal | 1.07 |
Attention
Maintaining Relevance | 6 | 3.2 | 15 | 8.06 | 67 | 36.02 | 37 | 19.8 | 61 | 32.7 | Normal | 1.1 |
The decision-making competencies | n | % | n | % | n | % | n | % | n | % | Mod | SS(±) |
Paying Attention to Data | 5 | 2.6 | 13 | 6.9 | 67 | 36.02 | 39 | 20.9 | 62 | 33.3 | Normal | 1.07 |
Independent Decision- 42 | 22.5 | 65 | 34.9 | 71 | 38.1 | 7 | 3.7 | 1 | 0.5 | Normal | 0.86 |
Decision-Making in Parallel with the 3 System | 1.6 | 6 | 3.2 | 49 | 26.3 | 45 | 24.1 | 83 | 44.6 | Very High | 0.99 |
Ability To Choose the 3 | 1.6 | 6 | 3.2 | 49 | 26.3 | 45 | 24.1 | 83 | 44.6 | Very High | 0.99 |
Making
Best Result
Under Pressure, Quick Decision-Making | 83 | 44.6 | 42 | 22.5 | 51 | 27.4 | 7 | 3.7 | 3 | 1.6 | Very low | 1.009 |
The motivation style competencies | n | % | n | % | n | % | n | % | n | % | Mod | SS(±) |
Career Planning | 8 | 4.3 | 4 | 2.1 | 54 | 29.03 | 38 | 20.4 | 82 | 44.08 | Very high | 1.1 |
![]()
By Creating a Warm, Positive Environment
5
2.6 15 8.06 135 72.5 29 15.9 2 1.07 Normal 0.62
By Supporting Social Opportunities
41 22.04 50 26.8 65 34.9 23 12.3 7 3.7 Normal 1.08
By Ensuring That They are Part of The Team
6 3.2 14 7.5 46 24.7 64 34.4 56 30.1 High 1.05
more collaborative leadership style, resonating with the relational and team-focused nature of nursing practice (32).
The distribution of general behavioural characteris- tics showed predominantly normal levels across most domains, indicating a balanced leadership group. Strengths such as patience, tolerance, and atten- tion to detail are particularly relevant to roles requir- ing emotional regulation and meticulous oversight. However, the low levels of self-motivation and inde- pendence among some leaders point to areas where additional organisational support could be benefi- cial. Research highlights that intrinsic motivation, resilience, and self-efficacy influence engagement,
satisfaction, and performance, particularly in high- stress clinical environments (1,30,33,34). This aligns with the present findings, suggesting opportunities to strengthen confidence and autonomous decision- making through targeted development.
Communication competencies showed clear strengths in factual, evidence-based communication, which sup- ports high-quality clinical practice and interdisciplinary coordination (34). Competencies such as influence, at- tentive listening, and maintaining relevance, however, demonstrated more balanced distributions, indicating variability that may benefit from focused communica- tion training. Effective communication remains one of the strongest predictors of collaboration, team cohe-
Table 5. The Management Competencies Distribution of Nurses | |||||||
The management competencies | Very Low | Low | Normal | High | Very High | ||
n % | n % | n % | n % | n % | Mod | SS(±) | |
Taking The Initiative 34 18.2 34 18.2 79 42.4 35 18.8 4 2.1 Normal 1.04
Awareness Of the Big Picture
9 4.8 30 16.1 51 27.4 71 38.1 25 13.4 Low 1.06
Combating Stress 62 33.3 59 31.7 45 24.1 16 8.6 4 2.1 Very low 1.04
Establishing Authority 3 1.6 27 14.5 136 73.1 15 8.06 5 2.6 Normal 0.6
![]()
Being Open to Innovation
42 22.5 66 35.4 71 38.1 6 3.2
1
0.5
Normal
0.8
Risk-Taking 84 45.1 42 22.5 52 22.9 6 3.2 2 1.07 Very Low 0.9
Delegating By Teaching 1 0.5 7 3.7 70 37.6 61 32.7 47 25.2 Normal 0.8
Long-Term Strategic Planning
3 1.6 6 3.2 51 27.4 44 23.6 82 44.08 Very High 0.9
![]()
Adding Excitement to Work
58
31.1 39 20.9 68 36.5 15 8.06 6
3.22
Normal
1.09
Business Discipline 4 2.1 6 3.2 49 26.3 45 2.4 82 44.08 Very High 1.01

Establishing An Emotional Bond with The Team
6
3.22 13 6.9 47 25.2 63 33.8 57 30.6
High
1.04
Effective Speaking and Leadership
41 22.04 50 26.8 65 34.9 23 12.3 7 3.7 Normal 1.08
sion, and patient safety (35,36), underscoring the im- portance of reinforcing these competencies.
Decision-making profiles reflected strong alignment with systematic, data-oriented approaches, as evi- denced by high scores in paying attention to data and system-parallel decision-making. These tenden- cies reflect a structured cognitive style that is well suited to the requirements of clinical leadership (36). However, the significant difficulty reported in quick decision-making under pressure suggests an area for improvement. Crisis decision-making, rapid risk assessment, and adaptive leadership skills are es- sential during periods of uncertainty or urgent clini- cal needs. Literature supports that transformational leadership behaviours and supportive work environ- ments can enhance rapid decision-making and critical thinking (37,38), pointing to a potential direction for leadership development initiatives.
Motivation-related competencies revealed strong ten- dencies in career planning and team inclusion, indicating a forward-looking mindset and commitment to maintain-
ing cohesive teams—both known predictors of engage- ment and retention (1,30,39,40). More balanced ratings related to social support suggest individual differences in how leaders cultivate social environments. Enhancing structured social opportunities may strengthen cohe- sion, morale, and workplace culture, aligning with evi- dence that supportive environments improve satisfac- tion and organisational commitment (16,41).
Management competencies demonstrated notewor- thy strengths in strategic planning, business disci- pline, and awareness of the broader organisational context, reflecting a strong strategic orientation among nurse leaders (11,42,43). However, lower scores in areas such as risk-taking, stress manage- ment, and initiative indicate developmental needs in adaptive and proactive leadership domains. These competencies are essential for navigating organi- sational change, leading innovation, and supporting staff in dynamic clinical environments (6,8). Enhanc- ing such competencies through structured leadership training, mentorship programmes, and resilience- building interventions could address these gaps.
Overall, the findings portray a highly competent and conscientious nursing leadership group with notable strengths in structure, planning, factual communica- tion, and strategic vision. However, important growth areas remain, particularly in rapid decision-making under pressure, self-motivation, risk-taking, and stress management. Addressing these areas through targeted leadership development and competency- based training programmes could enhance leader- ship effectiveness and organisational performance. Continued research into behavioural leadership pat- terns and competency development among nurse leaders will be essential for informing organisational policy, shaping leadership pathways, and supporting high-quality patient care.
This study has several limitations that should be con- sidered when interpreting the findings. First, the re- search was conducted within a single private health- care group and may not fully represent nurse leaders working in other organisational structures or public- sector settings, which limits generalisability. The data were collected through an online, self-report format, which may introduce response biases, including social desirability and self-enhancement tendencies that can influence personality and competency ratings.
The DISC behavioural assessment used in this study employs an ipsative, forced-choice scoring method, which does not permit traditional psychometric eval- uation such as Cronbach’s alpha. Similarly, the insti- tutional competency tool lacks published validity and reliability data, which may affect the interpretability and comparability of results.
The cross-sectional design captures behavioural tendencies and competencies at a single time point, preventing assessment of temporal changes or de- velopmental progress. Additionally, data collection occurred during the COVID-19 pandemic, a period characterised by increased workload and stress for nurse leaders, which may have influenced partici- pants’ behaviours, self-perceptions, and decision- making competencies.
Future studies should consider longitudinal designs, inclusion of multiple healthcare settings, and the use of psychometrically validated competency instru- ments to provide a more comprehensive and gener- alisable understanding of leadership behaviours in nursing.
![]()
![]()
This study provides a comprehensive overview of the behavioural tendencies and leadership competencies of an experienced nursing leadership workforce. The participants demonstrated notable strengths in con- scientiousness, strategic planning, and data-driven decision-making—competencies that are essential for effective leadership and high-quality management in contemporary healthcare settings. The predomi- nance of conscientious behavioural traits indicates a methodical, detail-oriented, and structured approach to leadership, while balanced communication and general behavioural characteristics suggest adapt- ability and strong foundational interpersonal skills.
Despite these strengths, the findings highlight several key areas for development, including rapid decision-making under pressure, self-motivation, and assertiveness in risk-taking. Addressing these gaps through targeted leadership development pro- grammes, mentorship, and competency-based train- ing has the potential to further enhance manage- rial effectiveness, strengthen resilience, and support high-performing clinical teams.
As healthcare environments grow increasingly com- plex, understanding the behavioural foundations of nurse leadership becomes critical. Investing in lead- ership development that aligns personality tenden- cies with organisational needs will not only support individual growth but also contribute to improved patient outcomes, stronger team dynamics, and sus- tainable organisational performance.
Conceptualisation: (SKA); Methodology: (SKA); Inves- tigation: (SKA); Writing—Original Draft Preparation: (SKA); Writing—Review and Editing: (SKA). All authors have approved the final manuscript.
The authors declare no conflicts of interest.
The author extends their sincere gratitude to all the participants who contributed to this study.
This research did not receive any specific grant from funding agencies in the public, commercial, or not- for-profit sectors.
![]()
![]()
Breed M, Downing C, Ally H. Factors influencing mo- tivation of nurse leaders in a private hospital group in Gauteng, South Africa: a quantitative study. Cura- tionis. 2020;43(1):a2011. https://doi.org/10.4102/ curationis.v43i1.2011
Asamani JA, Naab F, Ofei AMA. Leadership styles in nursing management: implications for staff outcomes. J Health Sci (El Monte). 2016;6(1):23–36. https://doi. org/10.17532/jhsci.2016.266
Bahlman-van Ooijen W, van Belle E, Bank A, de Man- Van Ginkel J, Huisman-de Waal G, Heinen M. Nursing leadership to facilitate patient participation in funda- mental care: an ethnographic qualitative study. J Adv Nurs. 2023;79(3):1044–55. https://doi.org/10.1111/ jan.15329
Bianchi M, Bagnasco A, Bressan V, Barisone M, Tim- mins F, Rossi S, et al. A review of the role of nurse le- adership in promoting and sustaining evidence-based practice. J Nurs Manag. 2018;26(8):918–32. https:// doi.org/10.1111/jonm.12638
Foots L, Swiger PA, Orina J, Campbell CM, Javed M, Hod- son P, et al. Recommendations from a systematic re- view of leadership development to support a new nu- rsing practice model. J Nurs Adm. 2023;53(12):661–7. https://doi.org/10.1097/NNA.0000000000001363
Alanazi FJ, Mersal FA. Achieving excellence: the role of leadership styles in fostering work performance and autonomy in nurses’ decision-making. 2024. https:// doi.org/10.21203/rs.3.rs-4427158/v1. Accessed Fe- bruary 20, 2025.
Baldino D. What is DISC? IMSTS. Available at: https:// www.imsts.com/what-is-disc. Accessed: 20.02.2025.
Underhil M. The relationships among situational lea- dership II, emotional intelligence and DiSC behaviour [Master’s thesis]. Cheney (WA): Eastern Washington University; 2015.
Herrity J. The 4 DISC personality types (plus 12 styles with careers). Indeed Career Guide. Available at: https:// www.indeed.com/career-advice/career-development/ disc-personality-types. Accessed: 20.02.2025.
Slowikowski MK. Using the DISC behavioural instru- ment to guide leadership and communication. AORN J. 2005;82(5):835–43. https://doi.org/10.1016/S0001-
2092(06)60276-7
Aini Q, Dzakiyullah NR, Abdulamir M. The use of the DISC personality test in assessing nurses’ personal charac- teristics. J Keperawatan Soedirman. 2023;18(2):111–8. https://doi.org/10.20884/1.jks.2023.18.2.6592
Shahzad K, Raja U, Hashmi SD. Impact of the five big personality traits on authentic leadership. Lea- dersh Organ Dev J. 2020;42(2):208–18. https://doi. org/10.1108/LODJ-05-2019-0202
Damti S, Hochman G. Personality characteristics as predictors of ethical leadership in regular times and in times of crisis. Sustainability. 2022;14(16):9800. https://doi.org/10.3390/su14169800
Peršolja M, Žvanut B, Rot Š, Markič M. Assesment of management styles among top nursing leaders in Slovenian primary health centres: a cross-sectional analysis. Leadersh Health Serv. 2024;37(5):157–68. https://doi.org/10.1108/LHS-10-2023-0083
Assiri MA. The big five personality traits and lea- dership practices of academic department chairs: a predictive study. Cent Educ Policy Stud J. 2024;15(3). https://doi.org/10.26529/cepsj.1736
Chen M., Wang A., Zhou B. Exploring core competenci- es of clinical nurses in Chinese tertiary hospitals: qu- alitative content analysis. BMC Nurs. 2023;22(1):166. https://doi.org/10.1186/s12912-023-01337-2
Kelagina G. A study on the effectiveness of the DISC personality test [Doctoral dissertation]. Selinus Uni- versity; 2021.
Mert-Karadaș M, Terzioğlu F, Koc G. Effects of persona- lity traits and leadership orientations of Turkish nur- sing students on their career adaptability: a cross-sec- tional study. Leadersh Health Serv. 2024;37(1):53–68. https://doi.org/10.1108/LHS-11-2022-0114
Nurochim AD, Wardani AA, Putri AR. Pembentukan dan perkembangan alat tes DISC: sexual literature review. Flourishing J. 2022;2(1):59–63. https://doi. org/10.17977/um070v2i12022p59-63
Barkhordari-Sharifabad M, Ashktorab T, Atashzadeh- Shoorideh F. Ethical leadership outcomes in nursing: a qualitative study. Nurs Ethics. 2018;25(8):1051–63. https://doi.org/10.1177/0969733016687157
Gómez PL, Barquero JD, Pestana JV. Evidencia empíri- ca del DISC en futuros líderes iberoamericanos. An Psicol. 2021;51(3):30855. https://doi.org/10.1344/ ANPSIC2021.51/3.30855
Fuqua RM, Bryan J. Leadership selection: DiSC results and leadership success in healthcare. Adv Soc Sci Res J. 2017;4(10):1–10. https://doi.org/10.14738/ assrj.410.3136
Purnamasari G. The Effectivness of Group communi- cation effectiveness using DISC measurement at PT ABC. Int J Res Publ. 2023;132(1):1–10. https://doi. org/10.47119/IJRP1001321920235444
Laschinger HKS, Wong CA, Macdonald-Rencz S, Burkoskı V, Cummings G, D’Amour D, et al. Part 1: The influence of personal and situational predictors on nurses’ aspi-
rations to management roles: preliminary findings of a national survey of Canadian nurses. J Nurs Manag. 2013;21(2):217–30. https://doi.org/10.1111/j.1365-
2834.2012.01452.x
Sukri U, Sari EC, Kailuhu CD. Pelatihan personal bran- ding and communication untuk meningkatkan percaya diri mahasiswa semester akhir di stak anak bangsa. J PKM Setiadharma. 2023;4(3):167–75. https://doi. org/10.47457/jps.v4i3.431
The PeopleKeys Store. DISC theory: understanding the DISC assessment. Available at: https://discinsi- ghts.com/pages/disc-theory. Accessed: 20.02.2025.
World Medical Association. World Medical Associa- tion Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–4. https://doi.org/10.1001/ja- ma.2013.281053
Holgaard R, Bruun B, Zingenberg F, Dieckmann P. Nurses and physicians conceptualising similar terms differently: an interview study. BMC Med Educ. 2024;24(1):698. https://doi.org/10.1186/s12909-
024-05682-x
Hosseini Moghaddam M, Mohebbi Z, Tehranineshat
B. Stress management in nurses caring for COVID-19 patients. BMC Psychol. 2022;10(1):124. https://doi. org/10.1186/s40359-022-00834-4
Cziraki K, Read E, Spence Laschinger HK, Wong C. Nu- rses’ leadership self-efficacy, motivation, and career aspirations. Leadersh Health Serv. 2018;31(1):47–61. https://doi.org/10.1108/LHS-02-2017-0003
Labrague LJ, Al Sabei S, Al Rawajfah O, Burney IA, Abu AlRub R. Factors associated with millennial nurses’ intention to pursue leadership roles. Leadersh Health Serv. 2024;37(2):215–30. https://doi.org/10.1108/ LHS-04-2023-0024
Pursio K, Kankkunen P, Sanner-Stiehr E, Kvist T. Pro- fessional autonomy in nursing: an integrative re- view. J Nurs Manag. 2021;29(6):1565–77. https://doi. org/10.1111/jonm.13282
Krczal E. Determinants of attractiveness of integra- ted care. J Health Sci. 2017;5(6):329-39. https://doi. org/10.17265/2328-7136/2017.06.008
Alhakami IY, Baker OG. Factors influencing nurses’ work motivation. Iris J Nurs Care. 2018;1(1):1–7. https://doi.org/10.33552/IJNC.2018.01.000503
Poortaghi S, Shahmari M, Ghobadi A. Exploring nur- sing managers’ perceptions of nursing workforce ma- nagement during the outbreak of COVID-19: a content analysis study. BMC Nurs. 2021;20(1):27. https://doi. org/10.1186/s12912-021-00546-x
Kim KJ, Yoo MS, Seo EJ. Exploring the Influence of Nursing Work Environment and Patient Safety Cul- ture on Missed Nursing Care in Korea. Asian Nurs Res. 2018;12(2):121–6. https://doi.org/10.1016/j. anr.2018.04.003
Lievens I, Vlerick P. Transformational leadership and safety performance among nurses: the mediating role of knowledge-related job characteristics. J Adv Nurs. 2014;70(3):651–61. https://doi.org/10.1111/ jan.12229
Hayati D, Charkhabi M, Naami A. The relationship between transformational leadership and work en- gagement in governmental hospitals nurses: a sur- vey study. SpringerPlus. 2014;3(1):25. https://doi. org/10.1186/2193-1801-3-25
Smith CM, Lane SH, Brackney DE, Horne CE. Mo- tivators and Success Strategies Experienced by Men in Nursing: An Interpretive Description Stu- dy. J Mens Stud. 2022;30(2):271–90. https://doi. org/10.1177/10608265211066096
Abu Yahya O, Ismaile S, Allari RS, Hammoudi B.M. Correlates of nurses’ motivation. Nurs Forum. 2019;54(1):7–15. https://doi.org/10.1111/nuf.12291
Wan Q, Li Z, Zhou W, Shang S. Effects of work envi- ronment and job characteristics on the turnover in- tention of experienced nurses: The mediating role of work engagement. J Adv Nurs. 2018;74(6):1332–41. https://doi.org/10.1111/jan.13528
González-García A, Pinto-Carral A, Pérez-González S, Marqués-Sánchez P. Nurse managers’ competencies: a scoping review. J Nurs Manag. 2021;29(6):1410–9. https://doi.org/10.1111/jonm.13380
Tolentino D, Sousa DRN, Melo NET. Metodología DISC: tendencias comportamentales en el ambi- ente de trabajo. RECIMA21 Rev Cient Multidiscip. 2023;4(11):e4114466. https://doi.org/10.47820/re- cima21.v4i11.4466 [Spanish]